Movement is one of the most characteristic features of living organisms. Chapter 17 of Class 11 Biology, Locomotion and Movement, explores the distinction between movement and locomotion, and examines how animals achieve various types of movements. The chapter explains the structure and functions of different types of muscles, the skeletal system in humans, the mechanism of muscle contraction, and the various types of joints that facilitate movement. It also covers different types of body movements and disorders related to the muscular and skeletal systems. This chapter is part of the comprehensive NCERT Solutions Class 11 Biology series, which covers all chapters in detail.
The NCERT Solutions for Locomotion and Movement provided here offer detailed, step-by-step explanations for all textbook questions, helping students strengthen their conceptual understanding, clear doubts effectively, and prepare efficiently for both school exams and competitive tests like NEET.
NCERT Solutions for Class 11 Biology Chapter 17 - All Exercise Questions
Q.
Draw the diagram of a sarcomere of skeletal muscle showing different regions.
Q.
Define sliding filament theory of muscle contraction.
Q.
Describe the important steps in muscle contraction.
Q.
Write true or false. If false, change the statement so that it is true.
(a) Actin is present in thin filament
(b) H-zone of striated muscle fibre represents both thick and thin filaments.
(c) Human skeleton has 206 bones.
(d) There are 11 pairs of ribs in man.
(e) Sternum is present on the ventral side of the body.
Q.
Write the difference between:
(a) Actin and Myosin
(b) Red and White muscles
(c) Pectoral and Pelvic girdle
Q.
Match Column I with Column II:
Column I | Column II |
(a) Smooth muscle | (i) Myoglobin |
(b) Tropomyosin | (ii) Thin filament |
(c) Red muscle | (iii) Sutures |
(d) Skull | (iv) Involuntary |
Q.
What are the different types of movements exhibited by the cells of human body?
Q.
How do you distinguish between a skeletal muscle and a cardiac muscle?
Q.
Name the type of joint between the following:-
(a) atlas/axis
(b) carpal/metacarpal of thumb
(c) between phalanges
(d) femur/acetabulum
(e) between cranial bones
(f) between pubic bones in the pelvic girdle
Q.
Fill in the blank spaces:
(a) All mammals (except a few) have __________ cervical vertebra.
(b) The number of phalanges in each limb of human is __________.
(c) Thin filament of myofibril contains 2 ‘F’ actins and two other proteins namely __________ and __________.
(d) In a muscle fibre Ca++ is stored in __________.
(e) __________ and __________ pairs of ribs are called floating ribs.
(f) The human cranium is made of __________ bones.
Download the PDF of NCERT Solutions for Class 11 Biology Chapter 17 –Locomotion and Movement
Class 11 Chapter 17 Biology Questions & Answers –Locomotion and Movement
Q1. Draw the diagram of a sarcomere of skeletal muscle showing different regions.
Solution: The diagram of a sarcomere of skeletal muscle showing different regions:
Q2. Define sliding filament theory of muscle contraction.
Solution: According to the sliding filament theory of muscle contraction, contraction of muscle fibres to produce contractile force takes place by the sliding of the thin filaments (actin fibres) over the thick filaments (myosin) found in the sarcomere of the muscle cell.
[Explanation: Sliding filament theory best describes the molecular basis of muscle contraction. It explains how myofibrils (actin and myosin) interact to produce contractile force. In sarcomere, actin forms thin filaments and myosin forms thick filaments. Sarcomere consists of two bands- A-band (Dark band) and I-band (Light band). A-band is the region of myosin thick filaments while I-band is the region of actin filaments which are not superimposed with myosin filaments. Actin filaments of I-band are connected to an elastic fibre called Z-line. There is a region in the central part of sarcomere that does not overlap with actin fibres is called H-zone. During the process of muscle contraction, thick filaments (myosin fibres, A-band) remains constant while thin filaments (actin fibres, I-band) change their length and slide over the myosin filaments. Actin filaments interact with the myosin head that results in pulling the actin filaments towards the centre of the sarcomere. In this process, length of sarcomere decreases and Z-lines of sarcomere come closer.]
Q3. Describe the important steps in muscle contraction.
Solution: Muscle contraction is explained by sliding filament theory. According to sliding filament theory, contraction of muscle fibers to produce contractile force takes place by the sliding of the thin filament (actin fibers) over the thick filaments (myosin) found in the sarcomere of the muscle cell. Important steps in muscle contraction are as follows:
1. Central nervous system sends signal for initiation of muscle contraction via a motor neuron.
2. Neural signal reaches motor end plate (the junction between a motor neuron and sarcolemma of the muscle fiber) and releases a neurotransmitter (acetylcholine) which generates an action potential in the sarcolemma that spreads through the muscle fiber and causes the release of calcium ions into the sarcoplasm.
3. Calcium ions bind to troponin that removes tropomyosin from the active sites of actin. These exposed active actin sites are now available to interact with myosin.
5. Heads of myosins form cross bridges by interacting with active sites on actin filaments and pull them towards the center of A-band by utilising the energy from ATP hydrolysis. Z line which is attached to actin filaments are also pulled inwards that shortens the sarcomere resulting in contraction. In this process, I-bands get shortened while the lengths of A-bands remain the same.
6. Myosin goes into relaxed state by releasing ADP and Pi. Cross bridge is broken. A new ATP binds to myosin and upon ATP hydrolysis next cycle of cross-bridge formation starts. This process continues till the calcium ions are sent back into sarcoplasmic cisternae that results into masking of active sites on actin filaments
Q4. Write true or false. If false change the statement so that it is true.
(a) Actin is present in thin filament
(b) H-zone of striated muscle fibre represents both thick and thin filaments.
(c) Human skeleton has 206 bones.
(d) There are 11 pairs of ribs in man.
(e) Sternum is present on the ventral side of the body.
Solution: (a) True
(b) False. H-zone of striated muscle fibre represents only thick filaments.
(c) True
(d) False. There are 12 pairs of ribs in man.
(e) True
Q5. Write the difference between :
(a) Actin and Myosin
(b) Red and White muscles
(c) Pectoral and Pelvic girdle
Solution: (a) Actin and Myosin
(b) Red and White muscles
| Red muscles |
White muscles |
| Red muscles are thin and smaller in size. |
White muscles are thick and longer. |
| Red muscles contain large amount of myoglobin that gives them reddish colour. |
White muscles contain lesser myoglobin. |
| Red muscles contain large number of mitochondria which are used for generating energy (ATP) to perform their function |
White muscles contain a smaller number of mitochondria |
| The contractions are slow but sustained over a longer period of time. |
The contractions are fast but of short duration |
(c ) Pectoral and Pelvic girdle
| Pectoral Girdle |
Pelvic girdle |
| Pectoral girdles help in the articulation of upper limbs. |
Pectoral girdles help in the articulation of upper limbs. |
| Pectoral girdle consists of two bones- Clavicle and Scapula |
Pelvic girdle is composed of three bones- Ilium, Ischium and Pubic. |
Q6. Match Column I with Column II :
Column I Column II
(a) Smooth muscle (i) Myoglobin
(b) Tropomyosin (ii) Thin filament
(c) Red muscle. (iii) Sutures
(d) Skull. (iv) Involuntary
Solution:
| Column I |
Column II |
| (a) Smooth muscle |
(iv) Involuntary |
| (b) Tropomyosin |
(ii) Thin filament |
| (c) Red muscle |
(i) Myoglobin |
| (d) Skull |
(iii) Sutures |
Q7. What are the different types of movements exhibited by the cells of human body?
Solution: Four different types of movements are exhibited by the cells of human body:
1. Amoeboid movement: This kind of movement is shown by specialised cells like macrophages and leukocytes in the blood which migrate from bloodstream to the site of injury to perform their function. These cells move by the formation of pseudopodia (streaming of cytoplasm) in the direction of movement. Microfilaments of the cytoskeleton are involved in this kind of movement.
2. Ciliary movement: Ciliary movement is shown by cells of the ciliated epithelium lining internal tubular organs. Cells present in the lining of trachea perform ciliary movement to sweep the dirt and mucus out of the lung. In females, the ciliary movement shown by the cells lining the fallopian tubes helps in moving ova from ovary to uterus. Cilia are also found in the cochlear cells of the ear.
3. Muscular movement: Muscle cells exhibit contraction and relaxation movement. This kind of movement is involved in moving our limbs, jaws, tongue, etc.
4. Flagellar movement: Sperms swim by means of flagellum which shows flagellar movement.
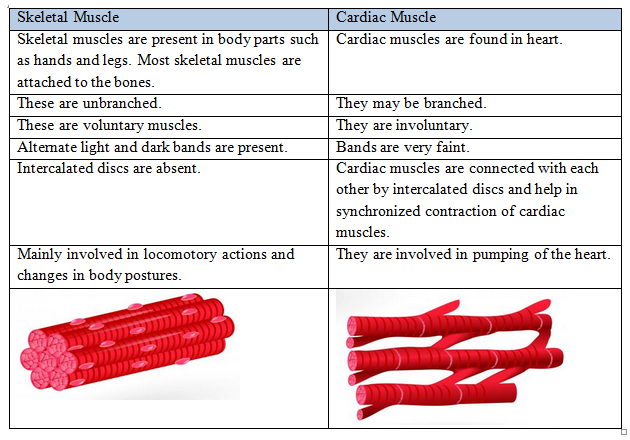
Q8. How do you distinguish between a skeletal muscle and a cardiac muscle?
Solution:
Q9. Name the type of joint between the following:-
(a) atlas/axis (b) carpal/metacarpal of thumb
(c) between phalanges (d) femur/acetabulum
(e) between cranial bones (f) between pubic bones in the pelvic girdle
Solution:
|
Bone |
Type of Joint |
| (a) |
atlas/axis |
Pivotal Joint |
| (b) |
carpal/metacarpal of thumb |
Saddle Joint |
| (c) |
between phalanges |
Hinge Joint |
| (d) |
femur/acetabulum |
Ball and socket Joint |
| (e) |
between cranial bones |
Fibrous joint |
| (f) |
between pubic bones in the pelvic girdle |
Cartilaginous joint (Pubic Symphysis) |
Q10. Fill in the blank spaces: (a) All mammals (except a few) have __________ cervical vertebra. (b) The number of phalanges in each limb of human is __________ (c) Thin filament of myofibril contains 2 ‘F’ actins and two other proteins namely __________ and __________. (d) In a muscle fibre Ca++ is stored in __________ (e) __________ and __________ pairs of ribs are called floating ribs. (f) The human cranium is made of __________ bones.
Solution: (a) All mammals (except a few) have seven cervical vertebra.
(b) The number of phalanges in each limb of human is 14.
(c) Thin filament of myofibril contains 2 ‘F’ actins and two other proteins namely troponin and tropomyosin.
(d) In a muscle fibre Ca++ is stored in sarcoplasmic reticulum.
(e) 11th and 12th pairs of ribs are called floating ribs.
(f) The human cranium is made of eight bones.
More Resources of NCERT Solutions for Class 11 Biology
NCERT Solutions for Class 11 Biology Chapter 17 – FAQs
1. What is the difference between locomotion and movement?
Movement refers to any change in position or place of any part of the body, such as bending of arms, beating of heart, or movement of food through the digestive tract. Locomotion is a specific type of movement where the entire body changes its position from one place to another, such as walking, running, swimming, or flying. All locomotion involves movement, but not all movements result in locomotion.
2. What are the three types of muscles found in the human body and their functions?
The three types of muscles are: (i) Skeletal muscles - voluntary, striated muscles attached to bones that help in body movement and locomotion, (ii) Smooth muscles - involuntary, non-striated muscles found in internal organs like the digestive tract, blood vessels, and urinary bladder that control internal movements, and (iii) Cardiac muscles - involuntary, striated muscles found only in the heart that pump blood throughout the body.
3. Explain the mechanism of muscle contraction (sliding filament theory).
Muscle contraction occurs through the sliding filament theory proposed by H.E. Huxley and J. Hanson. When a nerve impulse reaches the muscle fiber, calcium ions are released from the sarcoplasmic reticulum. These calcium ions bind to troponin, exposing binding sites on actin filaments. Myosin heads attach to these sites forming cross-bridges and pull the actin filaments towards the center of the sarcomere using ATP energy. This sliding of actin over myosin shortens the sarcomere, resulting in muscle contraction.